
Heartburn that won’t quit. A sour taste in your mouth when you wake up. Coughing at night that keeps you awake. If this sounds familiar, you’re not alone. About 20% of adults in the U.S. deal with GERD symptoms at least once a week. And while many turn to proton pump inhibitors (PPIs) for quick relief, the real key to lasting control isn’t just medication-it’s understanding how your daily habits shape what’s happening in your gut.
What GERD Really Is (And Why It’s More Than Just Heartburn)
GERD isn’t just occasional indigestion. It’s a chronic condition where stomach acid flows back into your esophagus because the lower esophageal sphincter (LES)-a muscular ring at the bottom of your food pipe-doesn’t close tightly enough. This isn’t a one-time glitch. It’s happening regularly, often twice a week or more. The acid burns the lining of your esophagus, which doesn’t have the same protective coating as your stomach. That’s what causes the burning, the regurgitation, and sometimes even a hoarse voice or chronic cough.
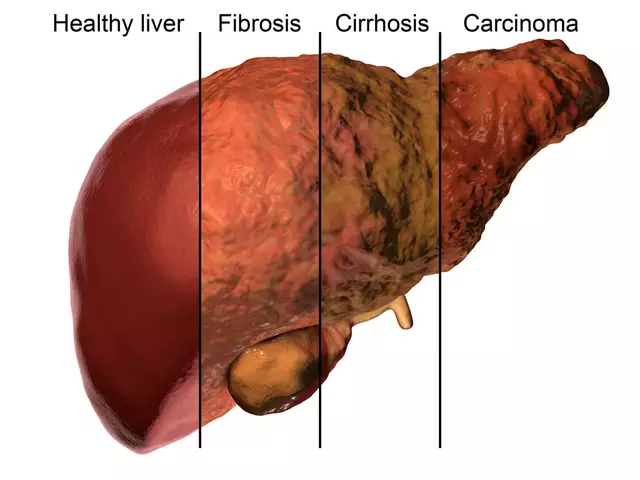
Left untreated, this constant irritation can lead to serious problems. Around 10-15% of people with long-term GERD develop Barrett’s esophagus, a condition that increases the risk of esophageal cancer. Others may end up with strictures-narrowing in the esophagus-that make swallowing painful or difficult. That’s why managing GERD isn’t just about feeling better today. It’s about protecting your long-term health.
PPIs: Powerful, But Not a Permanent Fix
Proton pump inhibitors like omeprazole, pantoprazole, and esomeprazole are the most effective drugs for reducing stomach acid. They work by blocking the final step of acid production in your stomach cells, cutting acid output by 90-98%. For someone with erosive esophagitis-visible damage in the esophagus-PPIs heal the tissue in 70-90% of cases. That’s why doctors often start with them.
But here’s the catch: PPIs don’t fix the broken valve. They just turn down the acid. And that’s where things get tricky. Studies show that 50-70% of PPI prescriptions are unnecessary. Many people take them long-term without ever reassessing whether they still need them. The FDA has warned about risks tied to prolonged use: a 35% higher chance of hip fractures in older adults after three or more years, a 20-50% increased risk of gut infections like C. diff, and potential vitamin B12 or magnesium deficiencies.
Worse, stopping PPIs suddenly can cause rebound acid hypersecretion. Your stomach, used to low acid levels, overcompensates and produces even more acid than before. This makes symptoms feel worse-so you think the PPI was working, when really, your body just went into overdrive. That’s why experts recommend trying to step down: switch to an H2 blocker like famotidine, or use PPIs only when symptoms flare up, not every day.
Lifestyle Changes: The Real Game-Changer
Here’s the truth most people don’t hear: losing just 5-10% of your body weight can cut GERD symptoms in half. That’s not a guess. It’s backed by clinical trials. Obesity puts pressure on the stomach, forcing acid upward. Even if you don’t see yourself as overweight, carrying extra weight around your midsection makes a big difference.
What you eat matters just as much. Coffee, tomatoes, alcohol, chocolate, fatty foods, and spicy meals are the top triggers-and they affect 70-80% of people with GERD. Cutting just coffee alone helps 73% of users. Eliminating late-night eating reduces nighttime acid exposure by 40-60%. That’s why doctors tell you to stop eating at least 2-3 hours before bed. Lying down with a full stomach is like tipping a bottle upside down.
Other simple fixes work too. Raising the head of your bed by 6 inches helps gravity keep acid where it belongs. Quitting smoking cuts GERD risk by half-it weakens the LES and increases acid production. Even wearing loose clothing around your waist can help. These aren’t just "tips." They’re evidence-based interventions that change the actual mechanics of reflux.

Why Lifestyle Alone Doesn’t Always Work (And What to Do About It)
Some people think, "I’ll just change my diet and skip the meds." But for many, lifestyle changes alone aren’t enough. A 2022 survey found that only 58% of users got moderate to complete relief from diet changes alone. Why? Because GERD isn’t always about what you eat. It’s also about anatomy. A hiatal hernia-where part of the stomach pushes up through the diaphragm-is present in 94% of people with erosive esophagitis. You can’t diet your way out of that.
Also, social life gets in the way. Who wants to say no to pizza at a friend’s party or wine at a dinner? That’s why successful management isn’t about perfection. It’s about awareness. Keep a food and symptom diary for two weeks. Note what you ate, when you ate it, and how you felt an hour later. You’ll start spotting your personal triggers. Maybe it’s not chocolate-it’s the garlic bread you eat with it. Or maybe it’s not the wine-it’s lying down 30 minutes after your last sip.
Apps like RefluxMD help track this. They let you log meals, posture, and symptoms. Over time, they build patterns you can’t see by memory alone. That’s how you move from guesswork to control.
The Smart Middle Ground: Combine Both Approaches
The best outcomes come from using PPIs and lifestyle changes together-but not forever. Start with lifestyle changes as your foundation. If symptoms persist after 2-4 weeks, add a PPI for 4-8 weeks to let your esophagus heal. Then, try to taper off. Switch to an H2 blocker on days you’re worried about symptoms. Or take the PPI only before big meals or events where you know you’ll eat trigger foods.
One study at Johns Hopkins showed that a 12-week structured program combining diet, weight loss, and sleep positioning led to 65% of participants stopping PPIs completely-without symptoms coming back. That’s not magic. It’s strategy.
And if you’ve been on PPIs for over a year? Talk to your doctor about a deprescribing plan. Many clinics now use automated alerts to flag long-term users and offer pharmacist-led reviews. You don’t have to keep taking something just because you started it.
When to Worry: Red Flags You Can’t Ignore
Not every heartburn needs a PPI. But some symptoms do. If you experience any of these, see a doctor right away:
- Difficulty swallowing or feeling like food gets stuck
- Unexplained weight loss
- Vomiting blood or passing black, tarry stools
- Persistent chest pain that feels like a heart attack
These aren’t normal GERD symptoms. They could mean complications like strictures, ulcers, or even cancer. An endoscopy might be needed to check your esophagus. Don’t wait. Early detection saves lives.
What’s New in GERD Treatment
The field is evolving. In 2023, the FDA approved Vonoprazan (Voquezna), the first new acid-blocking drug in 30 years. It works faster and may be more effective than PPIs for some patients. Endoscopic procedures like LINX®-a tiny magnetic bracelet placed around the LES-are helping people who can’t tolerate meds or want to avoid surgery. Another option, TIF (transoral incisionless fundoplication), rebuilds the valve from inside the esophagus without cuts or scars.
And AI is stepping in. Tools using machine learning are now predicting your personal triggers with 78% accuracy by analyzing your food logs and symptoms. Imagine getting a notification: "Your heartburn spiked after pasta last night. Try gluten-free noodles this week." That’s the future-and it’s already here.
Final Takeaway: You Have More Control Than You Think
GERD isn’t something you just live with. It’s not a life sentence of antacids and sleepless nights. You can take back control. Start with the basics: lose a little weight, stop eating before bed, cut your top triggers, and sleep with your head up. Then, use PPIs only as a short-term tool-not a daily crutch. Reevaluate every few months. Ask your doctor if you still need the medication. Track your symptoms. Learn your body’s signals.
Most people who stick with lifestyle changes see big improvements. And those who combine them wisely with medication don’t just feel better-they prevent long-term damage. You don’t need to be perfect. You just need to be consistent. Your esophagus will thank you.
Can I stop taking PPIs cold turkey?
No. Stopping PPIs suddenly can cause rebound acid hypersecretion, where your stomach overproduces acid and symptoms get worse. Instead, work with your doctor to taper off slowly-often by switching to an H2 blocker like famotidine for a few weeks before stopping completely.
Do I have to give up coffee forever?
Not necessarily. Coffee is a major trigger for 70-80% of people with GERD, but some find they can tolerate small amounts later on-especially if they switch to cold brew or low-acid beans. Try eliminating it for 2 weeks, then reintroduce it slowly. If symptoms return, it’s best to avoid it.
Is GERD caused by stress?
Stress doesn’t cause GERD, but it can make symptoms worse. It slows digestion, increases acid production, and makes you more sensitive to discomfort. Managing stress through sleep, exercise, or mindfulness can help reduce flare-ups-even if you’re still eating trigger foods.
Can children get GERD?
Yes. Infants often spit up, which is normal. But if a child over 1 year old has frequent vomiting, refuses to eat, cries during meals, or has chronic cough or wheezing, they may have GERD. Pediatricians can diagnose it and recommend safe lifestyle adjustments or medications.
How long does it take for lifestyle changes to work?
Most people notice improvement within 2-4 weeks of making changes like avoiding late meals, cutting triggers, and losing weight. But full healing of the esophagus can take 8-12 weeks. Be patient. Consistency matters more than speed.
Are natural remedies like apple cider vinegar helpful?
There’s no strong evidence that apple cider vinegar helps GERD. In fact, it’s acidic and may irritate the esophagus more. Some people swear by it, but it’s not backed by science. Stick to proven methods: diet, weight loss, timing meals, and medical guidance.
When should I consider surgery?
Surgery is usually considered only if lifestyle changes and medications fail, or if you have complications like a hiatal hernia or Barrett’s esophagus. Procedures like LINX® or fundoplication have high success rates-85-90%-but aren’t risk-free. Talk to a specialist if you’re thinking about it.
What to Do Next
Start today. Write down your top three trigger foods. Set a phone reminder to stop eating 3 hours before bed. Weigh yourself and set a realistic 5% weight loss goal. Then, schedule a chat with your doctor about whether you still need your PPI. You don’t have to fix everything at once. Small steps add up. And if you’ve been living with GERD for years, know this: relief is possible. You just need the right plan-and the courage to stick with it.




Kathy McDaniel
just stopped my ppi last month and holy crap the rebound was wild like my throat felt like i swallowed fire for a week but i stuck it out and now im coffee again and not dying lol
Anjula Jyala
the data is unambiguous ppi misuse is a public health crisis 50-70% of prescriptions are unnecessary and the rebound phenomenon is systematically ignored by primary care physicians who treat symptoms not pathophysiology the esophagus is not a landfill for pharmaceutical bandaids
Patrick Merrell
weight loss fixes everything but nobody wants to hear that because it means admitting you’ve been lazy for 10 years 🤷♂️
suhail ahmed
in india we call this aam pachak and the fix is simple ginger tea after meals and never sleep on a full stomach my grandma did this in 1972 and she’s still alive at 94 no ppi no problem
Candice Hartley
just started tracking my meals with refluxmd and already found out garlic bread is my trigger not the cheese 🤯
Marian Gilan
they dont want you to know but ppi’s are designed to keep you dependent the pharma companies know if you fix your diet you stop buying their drugs and thats why they push the daily pill narrative not the lifestyle fix
Harry Henderson
if you’re still on ppi after 6 months you’re not managing your health you’re outsourcing it to a pill stop being weak and get your life together your esophagus doesn’t care how busy you are
Paul Taylor
people think lifestyle changes are about willpower but its about environment if your kitchen is stocked with trigger foods your brain will always choose the easy path so remove the triggers before you even think about willpower its not about discipline its about design
also the bed elevation thing is real i put cinderblocks under my bed frame and suddenly i could sleep without waking up choking on acid like a horror movie
and dont get me started on the fact that most doctors dont even ask about meal timing they just write another script
you dont need a specialist you need a habit architect
and if you think apple cider vinegar works you’re just pouring acid on a burn
the science is clear but the system is broken
its not your fault its the ecosystem
but you can still fix it one meal at a time
start tonight
stop eating at 7pm
youll thank yourself in 3 weeks
Conor Flannelly
the real tragedy is that we treat GERD like a mechanical failure when its often a spiritual one
we eat too fast we eat while stressed we eat alone we eat to numb
the body remembers what the mind forgets
the esophagus is not just a tube it’s a messenger
its saying you are out of rhythm
the pill silences the message not the cause
in ireland we used to say if your stomach is angry your soul is hungry
maybe the answer isnt more acid suppression but more presence
Conor Murphy
just wanted to say thank you for this post i was on ppi for 4 years and thought i needed it forever
after 3 weeks of cutting coffee and eating before 8pm i havent taken one since
its not magic its just respect for your body
Murphy Game
they’re lying about vonoprazan too its just the next trap
they dont want you healed they want you subscribed
ai predicting triggers? that’s how they collect your data for insurance discrimination
the real cure is fasting and silence
and dont let them tell you it’s your fault
its the system